Ô‘◊≈‘…‘ÿ
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Chris Wilson 26 ·◊«’”‘ 2003, 01:37
|
Having used a lot of both,I definitely vote for antegrade nail.
You don't needlessly breach a joint, there are more size choices, distal locking is easier (the "distal" screws in a long retrograde nail being in the A/P orientation) and exchange nailing and reaming are easier.
In view of the segmental fragments a case could be made for unreamed antegrade nail, with a view to exchange nailing if there is delayed union.
Regards
Chris Wilson
Orthopaedic Surgeon
University Hospital
Cardiff
UK
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Ô‘–“¡◊…‘≈Ãÿ: Alexander Chelnokov 26 ·◊«’”‘ 2003, 02:26
|
THX for your comments. The nail is to be the same anyway - a UFN-like solid one. It can be inserted both ways, can't it? i also don't like to touch an intact joint. But reduction here looks easier with retrograde insertion so i expected maybe the approach is now strongly advocated...
:-)
|
[
Ô‘◊≈‘…‘ÿ ]
|
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Enes M. Kanlic 26 ·◊«’”‘ 2003, 02:07
|
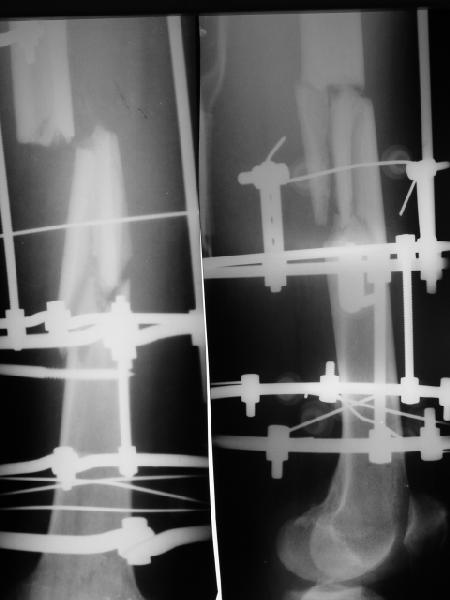
You did not tell us what was the reason to have circular ExFx frame on at the first place: any problems with soft tissues, any fractures around hip (proximal femur, acetabulum, pelvis, the size of patient (access to the piriformis fossa or greater trochanter), medical condition...!?
In general, it is risky (intramedullary infection) to have IM nail after pins transfixing the bone longer than 1-2 weeks (especially if it was any drainage around them and probably has to be after 6 weeks); it is better (not and easier; I prefer lateral decubitus) to avoid unnecessary violation of the knee joint (rare, but devastating complication of infection)...
Retrograde mostly if: distal fcatures, bilateral femur fractures, need for additional later proximal surgeries (acetabulum), polytrauma (abdominal, thoracic, neurowork), overweight and short patient (150 kg), soft tissue damage in hip area...
Sincerely
Enes M. Kanlic, M.D., Ph.D.
Associate Professor
Ortho Department at TTUHSC
El Paso, Texas
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Ô‘–“¡◊…‘≈Ãÿ: Alexander Chelnokov 26 ·◊«’”‘ 2003, 02:28
|
EKTE> You did not tell us what was the reason to have circular ExFx frame on at
EKTE> the first place: any problems with soft tissues, any fractures around hip
I suppose closed nailing was not available there, so they preferred ex-fix rather than open plating or plaster cast.
EKTE> In general, it is risky (intramedullary infection) to have IM nail after
EKTE> pins transfixing the bone longer than 1-2 weeks (especially if it was any
Our series of ex-fix to nail conversion now consist of more than 30 cases, and about 15 were acute conversion of fixators 3-11 months old with calm pin sites - no infection to date (knock-knock).
EKTE> Retrograde mostly if: distal fcatures, bilateral femur fractures, need for
Also ipsilateral femur+tibia. But AFAIR some colleagues in the list told about more excessive use of retrograde nails...
|
[
Ô‘◊≈‘…‘ÿ ]
|
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
James Carr 26 ·◊«’”‘ 2003, 02:08
|
I'll vote for antegrade as well. If you get a septic complication in a retrograde nail, the knee joint is a major problem. Jim Carr
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
V.M. Iyer 26 ·◊«’”‘ 2003, 18:08
|
I would certainly prefer an antegrade interlocking nail for the obvious reason. The proximal fragment will need reaming and can be done better from the pyriformis fossa than from below. From below means one has to go across the middle commin fragment, enter the prox fragment and then ream. There is n question of tossing a coin.
I presume you will take the precautions regarding the pin tracts of Iliz fixator
Dr V M Iyer
Iyer Orthopaedic centre Solapur India
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Ô‘–“¡◊…‘≈Ãÿ: Alexander Chelnokov 27 ·◊«’”‘ 2003, 10:06
|
OK, since voting was 5:0 for antegrade, the case has just been managed this way. Fixator appeared to be in malrotation about 40 degrees. Though some difficulties were met with gainig of proper length and pushing the nail beetwen parts of the comminuted fragment, the result seems satisfactory. THX!
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Ô‘–“¡◊…‘≈Ãÿ: V. M. Iyer 27 ·◊«’”‘ 2003, 18:25
|
I would like to know if 1) the proximal fragment was reamed, 2) which nail was used solid or cannulated and the size? 3) were you not worried about the potential for infection while doing nailing straightaway on removal of the fixator, 4) why not post the postop Xray.
Regards
V M Iyer
. Iyer Orthopaedic Centre,
103,Railway lines Solapur.413001.
|
[
Ô‘◊≈‘…‘ÿ ]
|
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Dr Harpal Singh Selhi 27 ·◊«’”‘ 2003, 09:25
|
From my experience spare the knee whenever possible
Prefer Antegrade nail
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
·Œ¡‘œÃ… Ï¡⁄¡“≈◊ 27 ·◊«’”‘ 2003, 09:40
|
≈“≈ÃœÕ ◊Ÿ”œÀ… Õœ÷Œœ … Œ≈ ‘“œ«¡‘ÿ ÀœÃ≈ŒŒŸ ”’”‘¡◊, ƒ¡ … €Ÿ‘ÿ— –œÕ≈Œÿ€≈ - “’À… Œ≈ Œ¡Õœ⁄œÃ…€ÿ.
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Ô‘–“¡◊…‘≈Ãÿ: Alexander Chelnokov 29 ·◊«’”‘ 2003, 16:49
|
Ó¡”fi≈‘ fi≈“≈⁄ ÀœÃ≈Œœ ÕŸ”Ãÿ ◊œ⁄Œ…Àá …⁄-⁄¡ ¬œÃ≈≈ »œ“œ€≈«œ ”œ–œ”‘¡◊Ã≈Œ…— Œ¡ Œ…÷Œ≈Õ –≈“≈ÃœÕ≈, fi‘œ¬Ÿ «◊œ⁄ƒÿ ”“¡⁄’ –œ€≈à Õ≈÷ƒ’ ”‘≈ŒÀ¡Õ… “¡⁄ÜաŒŒœ ‘“’¬À…. ˜ œ¬›≈Õ, … ⁄¡“’¬≈÷ŒŸ≈ ÀœÃÃ≈«… ¬ŸÃ… ≈ƒ…Œœƒ’€ŒŸ ”œ ”fi≈‘œÕ 5:0 ◊ –œÃÿ⁄’ ¡Œ‘«≈“¡ƒŒœ«œ, –œ‹‘œÕ’ ‘¡À … ”ƒ≈áÃ.
·Ï> ƒ¡ … €Ÿ‘ÿ— –œÕ≈Œÿ€≈ - “’À… Œ≈ Œ¡Õœ⁄œÃ…€ÿ.
· –œfi≈Õ’ –“… “≈‘“œ«“¡ƒŒœÕ €…‘ÿ— ¬œÃÿ€≈?
|
[
Ô‘◊≈‘…‘ÿ ]
|
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
M. Bryan Neal, MD 05 Û≈Œ‘—¬“ÿ 2003, 23:02
|
I favor antegrade approach.
retrograde in obese patients or polytrauma as you can operate on other injuries in one prep without repositioning on fracture table.
I find the biggest controversy to be the issue or immediate or delayed exchange given thin wires. What are you or did you do in terms of timing wire removal and rod insertion?
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
1100 W. Central Road, Suite 304
Arlington Heights, Illinois 60005
|
[
Ô‘◊≈‘…‘ÿ ]
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Ô‘–“¡◊…‘≈Ãÿ: Alexander Chelnokov 06 Û≈Œ‘—¬“ÿ 2003, 10:21
|
AAC> I favor antegrade approach.
As the case finally was done.
AAC> injuries in one prep without repositioning on fracture table.
We use only distractors for either.
AAC> exchange given thin wires. What are you or did you do in terms of
AAC> timing wire removal and rod insertion?
In the case half-pins/wires were removed while the nail was being inserted. Now 1 week postop - no signs of infection at the moment...
|
[
Ô‘◊≈‘…‘ÿ ]
|
|
Re: ·Œ‘≈- …Ã… “≈‘“œ«“¡ƒŒœ?
Fil 10 Û≈Œ‘—¬“ÿ 2003, 16:49
|
‰’Õ¡¿, fi‘œ Ã’fi€≈ ¬“œ”…‘ÿ ÕœŒ≈‘’, ‘¡À À¡À «Ã¡◊Œœ≈ ‘œ, «ƒ≈ œÀ¡÷≈‘”— ◊ ƒ¡ÃÿŒ≈ €≈Õ ”‘≈“÷≈Œÿ.
|
[
Ô‘◊≈‘…‘ÿ ]
|
( Ô‘◊≈‘…‘ÿ )
|