вверх
отправить
поиск
админ
главная
Предыдущее
Весь тред
|
Re: застарелое повреждение таза
Terry Finlayson 27 Март 2003, 17:04
|
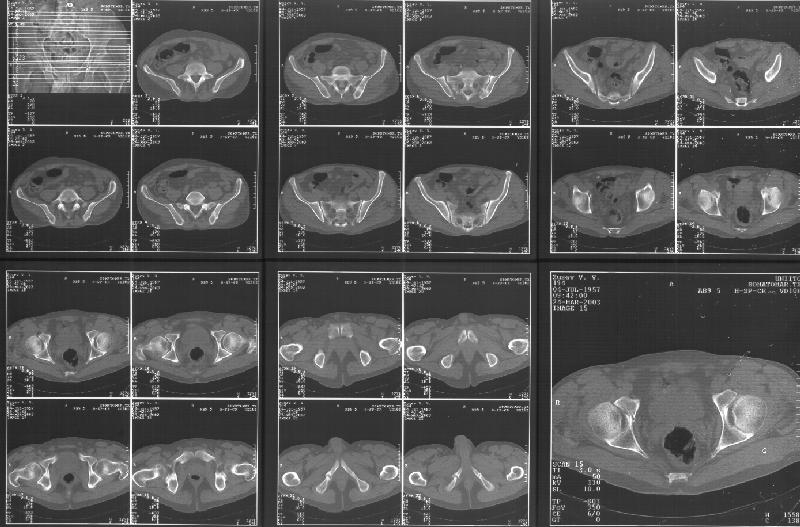
Based on the CT images you provided, he appears to have a nonunion of the the right ischium, which would explain his symptoms. General principles of treatment of hypertrophic (which this appears to be) nonunions suggest rigid fixation, but I'm not sure what the best approach would be. Could get a lag screw across the fracture through a Kocher-Langenbeck approach or plate osteosynthesis through direct ischial approach, but perhaps Chip, Adam or someone with more pelvic fracture experience could enlighten us all.
Terry Finlayson, MD
Alpine Orthopaedic Specialists
Logan, UT
|
|
|
Ответить
|
Re: застарелое повреждение таза
Chip Routt 27 Март 2003, 17:07
|
I didn't see it on the images...maybe I need glasses!!
I'll try to enlarge the images to understand.
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
|
[
Ответить ]
|
Re: застарелое повреждение таза
Отправитель: Adam Starr 28 Март 2003, 17:15
|
I didn't see it either - can anybody re-send me the CT images?
Presuming the patient DID have a nonunion of an ischial fracture, I'm not sure what the right course of treatment would be. You'd have to make yourself pretty darn sure that the symptoms were actually coming from the nonunion...and sometimes pain around the hip/butt is hard to
pinpoint.
If you decided that the pain and symptoms WERE due to a nonunion, then you'd have to talk with the patient about whether the treatment to fix
the nonunion would be worth it. Open reduction, plating and possible bone grafting of the ischium (presumably via a Kocher) is a pretty big
operation. The guy might decide the treatment is worse than the disease.
The option of percutaneous stabilization exists at a few centers, but I don't know that anybody has a big series of pelvic nonunions treated percutaneously so that we can say "this method works". There are a couple case reports in the literature.
I've done a number of sup ramus nonunions, and they seem to work okay.
I've treated one transverse acetabular fx nonunion percutaneously, and it worked - pain went away and the fx healed. But, that's just a
handful of anecdotes.
Adam Starr
Dallas, Texas
|
[
Ответить ]
|
Re: застарелое повреждение таза
Отправитель: Adam Starr 28 Март 2003, 17:25
|
Thanks for the link to the plain films and CT images.
I think this is just a pelvic ring disruption that has gone on to a non-union. The arrow is pointing to the inferior ramus non-union, and
the sup ramus is a high "root" fracture, right near the pecten. The sup ramus fracture enters the tab - you could call it an acetabular
fracture - but down here in Dallas we treat these acutely as stable pelvic ring injuries. The fracture in the anterior portion of the
acetabulum is so low it doesn't seem to cause much trouble.
His R sacroiliac joint is opened anteriorly a little bit - the "unreduced posterior lesion" Alex mentioned in his first post. My earlier post about plating, bone grafting, etc., is all wrong.
What you have is a pelvic fracture that hasn't healed after 4 months or so, with a minimal deformity.
I think what I would offer the guy is a percutaneous iliosacral screw to stabilize and improve the SI joint alignment, coupled with a perc anterior column screw to stabilize the high ramus fx. These screws aren't easy to place, and have a host of potential problems and complications. But, I think they would work.
The open treatment options carry more morbidity, in my opinion, but they could achieve the same result. It's possible to do an ilioinguinal
approach and stabilize both fractures. Bone grafting of each site (you would probably aim for a fusion of the SI joint if you chose the open route) and plate fixation would likely lead to union.
The perc screw method would also likely lead to union, but with less surgical dissection. The problem with the perc method is that it
requires an expert fluoroscopy technician, and a surgeon who understands the anatomy, as seen on fluoro. It's hard to do.
Adam Starr
Dallas, Texas
|
[
Ответить ]
|
Re: застарелое повреждение таза
Отправитель: Alexander Chelnokov 28 Март 2003, 17:28
|
B> Re case: http://www.hwbf.org/hwb/conf/alex47/pelinj.htm
BB> You can see the images - albeit small - (if the server holds out - it has
A link to "full-size" image (scanned with 300 dpi resolution to 2776x1832 pixels, ~900kb) is
http://weborto.net/forum/1048138303/pics/2k30326i
Thanks for advices.
--
Best regards,
Alexander N. Chelnokov
|
[
Ответить ]
|
|
( Ответить )
|
|





{kind=link}
{kind=link}